
Osteogenesis Imperfecta
Understanding the medicine behind O.I

“My baby's bones are breaking inside of my belly, the place he's supposed to be safe?”
These were the devastating words of Sarah Drew as April Kepner in Grey's anatomy. As a fan and lover of medical rom-com, my heart easily inclined to Grey’s Anatomy but no one prepared me for the many medical plot traumas. In Season 11, Episode 11, “All I Could Do Was Cry,” I watched one of the most heartbreaking scenes involving one of my semi-favorite characters, April Kepner reacting to the news of her baby boy being diagnosed with Osteogenesis Imperfecta type II, the lethal form. The diagnosis didn’t come all at once. April had gone for her routine ultrasounds, the same way every expectant mother does, hopeful, excited, watching tiny limbs move across the screen. Everything seemed fine, or at least not alarming enough to raise suspicion.
Not until an ultrasound was performed and that was when Dr. Nicole Herman, Grey Sloan Memorial’s renowned fetal surgeon, was brought in and suddenly, April found herself being told that her baby’s bones were so fragile they were breaking inside her womb. But beyond the drama lies an important question:
What exactly is Osteogenesis Imperfecta, and why does it make the bones so fragile, even before birth?
According to global health references such as the World Health Organization (WHO), Osteogenesis Imperfecta (OI) is defined as a group of rare genetic disorders characterized by impaired collagen production, leading to fragile bones that fracture easily, often with minimal or no trauma.

In simpler terms, OI is a condition where the body cannot make strong, healthy collagen, the protein that gives bones their strength and structure. Without enough normal collagen, the bones become thin, brittle, and prone to breaking, sometimes even before a baby is born. A child with OI is born with bones that are much more fragile than normal. Think of bones like building blocks: in most people, the blocks are strong and tightly packed. In OI, the blocks are there, but they’re not as strong as they should be, so they crack more easily. With that said, it’s important to understand that:
It’s genetic. The baby is born with it.
It’s nobody’s fault. Not the mother, not the father.
It doesn’t mean the child can’t live a full life. It just means their bones need extra protection and special care.
But hold on a minute.
If you watched the episode, you might be thinking: “Then why didn’t April’s baby survive? Why was his case so severe?”

That’s where the truth April faced became heavier. Osteogenesis Imperfecta isn’t just one condition, it has different types, and each type behaves differently. Some are mild. Some are manageable. Some are barely noticeable in everyday life. And then… there’s the form that April’s baby had.
Because her baby had Type II.
Now, Type II is the most severe form of osteogenesis imperfecta. Babies with this type have bones so fragile that fractures can happen before birth. Their ribs, their spine, their limbs that many of them break while the baby is still in the womb. The chest can become too small to let the lungs grow, making it difficult, and sometimes impossible, for the baby to breathe after delivery. To really understand why some children live long healthy lives with OI and why April’s outcome was so painful, it helps to look at the four main types.
The Types of Osteogenesis Imperfecta
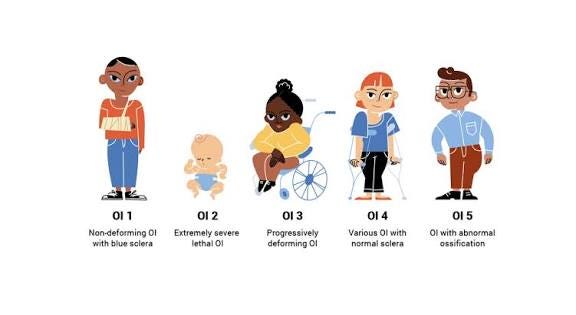
Type I Osteogenesis Imperfecta : This is the mildest form of brittle bone disease. Children with this type have bones that break more easily than normal, but they usually grow at a typical rate and can live active, full lives with some extra care. It is genetic, caused by a change in a gene that makes collagen, the protein that strengthens bones, and is not the result of anything a parent did. Some signs include a slight blue tint in the whites of the eyes, brittle or discolored teeth, and in some cases, hearing loss later in life. Despite these differences, children with Type I generally look like any other child and can participate in most everyday activities safely.
Type II OI: is the most severe and devastating form of OI. Babies with this type have bones so fragile that fractures can occur even before birth, inside the womb. The ribs and chest often do not develop properly, making breathing after birth extremely difficult, and sadly, survival is very rare. This is the type April Kepner’s baby had, and it explains why the diagnosis was so heartbreaking. Like all forms of OI, it is genetic and caused by a problem with collagen production, but the severity makes it life-threatening from the very beginning.
Type III is a severe form that is survivable. Children are born with multiple fractures and may develop bone deformities over time. Their growth is often affected, and they may need wheelchairs, braces, or other support to move safely. With attentive medical care and support, children with Type III can live into adulthood, though their bones remain very fragile.
Type IV is moderate in severity. Children with this type experience fractures and may have some deformity or shorter stature, but their condition is less severe than Type III. Most children with Type IV can lead active lives with careful management, including protective measures, physical therapy, and regular medical follow-up.
Type V Osteogenesis Imperfecta is a rarer form of the condition. Children with this type also have fragile bones, but what makes it different is a specific pattern in how the bones form and heal. For example, some bones may develop unusual calcifications or extra bone growth in certain areas, which can affect movement. Fractures still happen, and growth may be affected, but with proper medical care, children with Type V can often lead active lives.
Detecting Osteogenesis Imperfecta before a baby is born can be challenging, especially in the early stages of pregnancy. That’s why April Kepner kept going back for ultrasounds, each time hoping for reassurance, each time wondering if something was wrong. In reality, some signs of OI simply aren’t visible until the bones have grown enough to be seen clearly on a scan. By mid-pregnancy, usually around 18 to 22 weeks, ultrasounds can reveal clues. Doctors look for bones that are unusually short, bowed, or fractured, as well as a chest that may be smaller than expected.
To confirm a diagnosis, specialists can also use genetic testing. Tests like amniocentesis or chorionic villus sampling allow doctors to examine the baby’s DNA for changes in the genes responsible for collagen production. These tests provide certainty, but they are only done when there is a strong reason to suspect a condition like OI. When it comes to surgery for Osteogenesis Imperfecta, the possibilities depend entirely on the type and severity. For mild or moderate forms, like Type I or IV, orthopedic surgeries can help straighten bones, fix fractures, and improve mobility. Surgeons can insert metal rods into long bones, repair deformities, and help children lead more active lives.
But in Type II, the situation is far more complicated. Because the bones are extremely fragile, even before birth, surgical options are extremely limited. The chest may be too small to support breathing, and fractures can happen spontaneously. Unfortunately, this means that many babies with Type II cannot survive long enough after birth for corrective surgeries to be possible. The medical team focuses on comfort care and supportive measures, rather than attempting high-risk interventions.
Understanding OI is not just about recognizing its medical challenges—it’s about empathy, awareness, and support for those affected. By learning more, sharing knowledge, and advocating for research and better care, we can help families and children with OI live safer, fuller lives. Awareness is the first step; compassion and action are what follow.